
Report of Office of Polar Programs Subcommittee on USAP COVID Protocols
May 1, 2023
Executive Summary
The COVID-19 (SARS-CoV-2, hereafter referred to as COVID or COVID-19) pandemic was an unprecedented global emergency that threatened the overall success of the mission of the United States Antarctic Program (USAP). The last few years of risk mitigation been extremely challenging yet successful at keeping COVID out of USAP stations, but accomplished at the expense of deprioritizing science. COVID management in Antarctica is confounded by the extreme austere environments in which people are required to live and work while supporting the USAP, and a further challenge is the constant movement of South Pole and deep field participants through the large McMurdo Station community. While morbidity and mortality due to COVID have decreased significantly, the virus continues to circulate globally. The goal of this Subcommittee was to discuss the current state of the COVID pandemic, the potential continued threats to the mission of safely achieving science goals in Antarctica, and to discuss, plan, and introduce recommendations to provide the ability to protect to the maximal effect the supporting personnel of the mission, while also trying to maximize the flexibility and resources needed to accomplish the science mission.
The potential for a local outbreak, the decreased ability to treat and/or evacuate a patient, and experience that some disease mitigation efforts can result in significant disruptions to the scientific mission without improving disease outcomes require that USAP enact logical and actionable COVID mitigation protocols.
The Subcommittee is in agreement that the NSF/USAP is justified in its approach for accomplishing US national science goals in Antarctica and decreasing delays to funded science projects while mitigating undue health impacts for deploying USAP participants. The Subcommittee has a range of recommendations (bolded throughout the remaining text) for additional measures and/or considerations with respect to the draft USAP COVID Management Plan presented by NSF. These include:
- Recommending all USAP deployers be up to date with COVID vaccines, including boosters, according to CDC guidance
- Considering allowing deep field camps (particularly WAIS Divide) to accommodate isolation of asymptomatic or mildly symptomatic vaccinated COVID-positive participants including providing supplemental lodging and clinical resources
- Introducing air filtration in indoor station environments
- Consider introducing targeted wastewater surveillance
- Forward planning so that COVID management evolves into general infectious disease management in future years
- Clear, consistent, and frequent communication of plans to all stakeholders in settings ranging from camps and stations to NSF leadership (Office of Polar Programs and Office of the Director), science teams (e.g. “grantees”), contractors, Air National Guard, etc.
Introduction
The Subcommittee (see full list of members in Appendix 1) met together with NSF Office of Polar Programs leadership on April 24 and April 25, 2023. On the first day of the meeting, presentations from NSF personnel provided background information on the USAP and its operations since the start of the COVID pandemic in 2020. The material presented included an overview of the COVID protocols implemented in the past three seasons, as well as a description of the operational and scientific impacts caused by these measures. On the second day of the meeting, presentations and discussions focused on the proposed protocols to be implemented in the 2023-24 austral summer season. Led by chair Dr. Peter Neff, the Subcommittee collaborated on this report for the remainder of the week of April 24, 2023, delivering a final draft on May 1, 2023.
Charge
The Subcommittee, gathered by the NSF Advisory Committee for Polar Programs, was charged to “review the drafted COVID posture and provide additional recommendations to reduce the risk COVID presents to the logistical operations and science support of the USAP, operated by the Office of Polar Programs, Directorate for Geosciences.” Additionally, the objectives and scope of the subcommittee were to “provide advice and recommendations concerning the USAP development and implementation of health protocols in response to COVID in USAP-operated sites in Antarctica.” The complete subcommittee charge can be found in Appendix 2.
General Response to Charge
Overarching goals of the NSF/USAP COVID mitigation and control plan include:
- To minimize, not eradicate, the introduction and spread of COVID at NSF stations, vessels, and camps in Antarctica.
- OPP should rely on best available evidence and science as well as the most up to date and applicable guidance from the Centers for Disease Control and Prevention (CDC), National Institutes of Health (NIH), World Health Organization (WHO) and other reputable bodies to design and implement prevention and mitigation protocols.
- To rely on data, best practices and guidance that best represent local conditions, population-specific risks and organizational/logistical/resource limits in designing protocols.
- To minimize disruption to scientific endeavors due to COVID (and other communicable disease) related to:
- morbidity and/or mortality
- unattainable or unduly burdensome mitigation and control efforts
- unacceptable impacts to the ability of South Pole and deep field science and support teams to accomplish science goals
- Antarctica is an austere environment that requires much advance planning to operate in. Different work areas have added challenges. Protocols should:
- be based on the understanding that abrupt and significant changes can result in significant and variable operational challenges that are site-and season-dependent; and
- account for the specific risks associated with severe disease in areas with least access to adequate clinical care.
Specific clinical and public health recommendations
Protocols will rely on a combination of vaccination, isolation, use of respirators, testing and improving indoor air quality to maximize the safety of personnel and achieve the goals of the organization. Based on the remoteness, operations, and lifestyle of USAP participants at McMurdo Station, the CDC’s guidelines most applicable to working and living conditions present on Antarctica form the basis for the following recommendations.
- Vaccination: Being the most reliable defense against severe COVID disease, we recommend:
- mandating that all participants are “up to date” according to the latest CDC recommendations https://www.cdc.gov/vaccines/covid-19/clinical-considerations/interimconsiderations-us.html
- establishing a waiver system to allow review of individual cases who cannot comply with the vaccine mandate; and
- ensuring on-site vaccine supply is readily available to allow for ongoing compliance with the vaccine mandate
- Isolation and use of respirators and barrier face coverings: Isolation and the use of respirators and barrier face coverings (BFCs) is a critical component of our efforts to decrease the spread and impact of COVID and other respiratory illnesses on science operations in Antarctica. The panel recommends:
- Mandated respirator use periods
- During isolation period (isolation defined as removing this person from the population as much as is feasible after a positive COVID test) it is expected for infected individuals to follow the CDC isolation guidelines as closely as possible which suggest strict isolation from days 0-5, with free movement while wearing a respirator in shared indoor public spaces on days 6-10.
Given the unique operational considerations and science imperative of work in Antarctica, the panel recommends modification to the CDC recommendations:- NSF should require the use of a NIOSH Approved® N95® filtering facepiece respirator (N95 respirator) for all staff who must exit isolation through day 10 in place of a mask of lower quality.
- In consultation with the responsible clinical and public health personnel, the panel also recommends on a case by case basis permitting individuals who are needed for essential work functions before day 6 after a COVID diagnosis may leave isolation for these functions as long as they are wearing an N95 respirator in shared spaces or are able to work solo or outside.
- Respirator mandates can be increased by clinical and public health officers as needed and in response to increased rates of local transmission or based on results of environmental testing or other monitoring. NSF should consult with the Occupational Safety and Health Administration (OSHA) to determine the applicability of the Respiratory Protection Standard when requiring the use of respirators for respiratory protection from COVID.
- During isolation period (isolation defined as removing this person from the population as much as is feasible after a positive COVID test) it is expected for infected individuals to follow the CDC isolation guidelines as closely as possible which suggest strict isolation from days 0-5, with free movement while wearing a respirator in shared indoor public spaces on days 6-10.
- Recommended respirator or BFC use periods
- Periods of transit or travel: Travel on any form of public or group transportation poses a heightened risk for acquiring COVID and other respiratory infections. To decrease the chance of disrupting activities on Antarctica due to increased incidence of symptomatic, especially serious illness, we strongly suggest all personnel consider using a respirator or BFC:
- as part of increased protection against all respiratory infections in public settings for 5 days prior to deployment; and
- on all forms of public transportation (e.g. planes, buses) and transit points (e.g airports) on all legs of the journey to gateway cities. (Gateway cities: i.e., Christchurch, New Zealand or Punta Arenas, Chile)
- Upon arrival and before transfers, all personnel are encouraged to maximize the use of respirators or BFCs when in shared spaces for the:
- first 5 days after arrival on ice;
- 5 days prior to deploying to field sites; and
- 5 days after arrival to field sites
- Respirator selection:
- The panel recommends requiring a NIOSH Approved® N95® filtering facepiece respirator for mandatory use periods.
- The panel recommends offering N95 respirators, KN95 filtering facepiece respirators, or BFCs for recommended use periods outside of mandatory respirator use periods. Alternatives, such as surgical masks are less effective but their use is left to the discretion of individuals.
- Respirator supply:
- For a list of N95 respirators, see the NIOSH Certified Equipment List at https://www.cdc.gov/niosh/npptl/topics/respirators/disp_part/N95list1.html. For a list of BFCs, including Workplace Performance Plus models, see the NIOSH PPE-Info page at https://wwwn.cdc.gov/PPEInfo/RG/FaceCoverings. FDA provides a description of these products at https://www.fda.gov/medicaldevices/personal-protective-equipment-infection-control/n95-respiratorssurgical-masks-face-masks-and-barrier-face-coverings#face-masks.
- Indoor Air Quality (IAQ): Maintaining indoor air quality (specifically, here, reducing the concentration of airborne pathogens in close living quarters) in Antarctica presents unique challenges. We suggest that NSF engage appropriate experts to investigate applicable methods for maximizing indoor air quality on Antarctica. Even when increasing air turnover is difficult because of the cold environment, air filtration can be introduced with minimal expense. There is substantial science on air filtration that has emerged since late 2020, and these systems have been implemented around the world.
- Testing:
- Of individuals:
- Rapid Antigen Tests (RAT) should be made freely available to all personnel for self-testing when first symptomatic.
- All symptomatic individuals should seek advice from a clinician.
- Clinicians should have the ability to provide supervised RAT or PCR testing.
- Clinicians should have the ability to provide anti-viral and other therapies per current CDC standards.
- Option to test personnel with Biofire respiratory panel to evaluate for RSV and/or Influenza.
- Routine testing of asymptomatic persons in Antarctica is not recommended.
- Environmental:
- Environmental surveillance should be considered as a complement to other strategies at the discretion of relevant clinical and public health personnel.
- Of individuals:
- Periods of transit or travel: Travel on any form of public or group transportation poses a heightened risk for acquiring COVID and other respiratory infections. To decrease the chance of disrupting activities on Antarctica due to increased incidence of symptomatic, especially serious illness, we strongly suggest all personnel consider using a respirator or BFC:
- Mandated respirator use periods
Plan must clearly outline individual and organizational duties and responsibilities
- Justify the plan in terms of risks and benefits to the individual, the organization, and the science mission.
- Outline consequence for variance from protocols and responsibilities.
Establish culture of transparency, open communication and shared risk/responsibility
- Plan should respect the priorities, constraints and “shared reality” of participants.
- Plan should also make clear the particular needs of science and support teams who must move safely and effectively through McMurdo Station and on to field sites including South Pole Station, WAIS Divide, etc. Additional designs with this in mind are needed, including the ability to isolate COVID-positive asymptomatic or mildly symptomatic participants at large deep field camps such as WAIS Divide, rather than add a lengthy and resource intensive medical evacuation to McMurdo Station (for location overview, see map in Appendix 3).
- Must incorporate a robust communication strategy to disseminate plans and answer questions/address concerns from multiple stakeholders. This must include regular and recurring communication, utilizing various methods, to set appropriate expectations about the inherent risks of operating in an austere location, the layered approach that USAP is taking to mitigate the risk of infectious diseases while prioritizing the science mission, and the personal responsibility to follow these protocols in order to meet shared organizational and scientific goals. Ask science and workcenter group leaders to discuss with teams prior to arrival.
- Repeat consistent message in many settings, from multiple messengers at multiple levels of authority across NSF, Antarctic Support Contract (ASC), science groups, Air National Guard etc.
- Use infographics in communication at stations and camps, and in email and other communications with all stakeholders and USAP participants.
- Plan should encourage USAP participants to feel that they can report feeling ill in order to implement measures to protect the community and their team members (without fear of overly burdensome impacts to work and science). This plan can take many forms but should allow for the following outcomes:
- the ability for members who work in worksites that allow for isolation (ex: heavy machinery operators) to continue working while in isolation if asymptomatic or only mildly symptomatic;
- administrative functions that can be performed from isolation sites (provide laptops as needed, desks, chairs and wireless internet access in isolation dorm rooms at McMurdo/South Pole);
- a preventative assessment and mitigation of risk of “single failure” jobs that could stop operations if individual was to become ill with an infectious disease;
- appropriate “float” days built into schedules to account for risk; and
- the ability to manage identified asymptomatic or mildly symptomatic COVID cases at deep field sites (i.e. isolation or continued work while masked and distanced from others) without medical evacuation back to McMurdo Station.
The COVID mitigation and response plan should be applicable to control of other infectious diseases.
Specific Responses to Key Questions
- What are the primary risks that COVID-19 presents to the deployed USAP community, and how do those risks compare with other safety and health risks in Antarctica?
All infectious diseases pose variable morbidity and mortality risks to affected individuals and differing risks for transmission based on population and environmental characteristics. COVID is one of numerous diseases associated with airborne spread. https://www.ncbi.nlm.nih.gov/books/NBK531468/ During times of increased global incidence of disease (as during the peak of the COVID pandemic), the risk of transmission is increased. Current global incidence of COVID is decreased. Likewise, risk of serious illness has been decreased due to vaccine and disease associated immunity. COVID-19, as a novel coronavirus, was also associated with serious illness when compared with endemic coronaviruses. In short, compared to other airborne viruses that might pose safety and health risks in Antarctica, COVID has a diminishing but present risk of producing symptomatic illness that could affect the deployed USAP personnel and viability of projects.
The primary risk due to COVID is the occurrence of a local outbreak which could result in an inability to interrupt local disease transmission resulting in an increase of symptomatic cases with associated increase in illness and possibly death. In addition, an outbreak of COVID in Antarctica has the potential of significantly and even irreversibly impacting some of USAP’s science imperatives by resulting in multiple, simultaneously ill personnel and predictable negative impacts to operations and progress towards season science goals. Even one very sick individual can consume large amounts of healthcare and logistical resources that not only impact the well-being of the person but can affect multiple programs. A Prolonged evacuation of incapacitated individuals could add to the risk, consuming finite resources and imparting delays that may severely limit science success. Lastly, not enough is known about the chronic infection or symptoms that exist postinfection, commonly called “Long COVID”. Thus, a focused, well-thought out risk mitigation plan for COVID is essential. We also agree that such a program will help mitigate the introduction and spread of other infectious diseases on Antarctica.
In unvaccinated individuals, especially those with no previous natural immunity, COVID poses grave risk of severe disease and death that may require medical resources beyond those available in Antarctica. Compared to other infectious disease risks faced by USAP staff, even in vaccinated individuals, COVID still causes more morbidity and mortality in the workforce age group than other common infectious diseases, such as Influenza and RSV, at the time of this report. However, it should be noted that any infectious disease could pose a future risk that would surpass even the COVID pandemic issues.
USAP personnel with chronic disease burden and unanticipated worsening of their underlying condition also pose a safety and health risk. This is in addition to existing risk of unanticipated medical emergencies, such as heart attack, stroke, and acute surgical emergencies, and are still more likely to challenge the medical team at a rate possibly exceeding the COVID risk. Because the area of operation is very austere and often subject to unpredictable weather patterns, this risk of morbidity and mortality from environmental factors is also likely similar to the COVID risk for generating unplanned evacuations. Lastly, traumatic injury is still the most likely event to trigger an unplanned evacuation from the area.
Are NSF’s goals for COVID-19 management during the 2024 season appropriate and achievable?
NSF’s goal is to ensure the health and safety of USAP deployers while they accomplish the important scientific research in Antarctic research stations, camps, and transport vessels.The NSF’s strategies to accomplish this are to implement measures to minimize transmission of infection and to proactively prevent negative health outcomes of infected individuals while ensuring the optimal implementation of the Antarctic scientific agenda. The Subcommittee agrees that these goals are generally appropriate and achievable, with a few recommendations to avoid undue impact on USAP participant health and science goals.
The goals reflect a shift from the “no-COVID” policy at the start of the pandemic, and maintained by USAP through the 2020-2021 and 2021-2022 Antarctic summer seasons with near-total reduction in the scope of science accomplishments, to an acknowledgment that COVID is now endemic globally and can be pro-actively managed using evidencebased strategies to minimize transmission and risk of severe disease. The panel did identify some areas of CDC recommendations that could enhance the stated plan (e.g. ventilation) that if implemented would complement the proposed plan.
These goals and the proposed COVID-19 management plan do leave unresolved challenges such as how to position McMurdo, Palmer, and South Pole stations for winter operations after the 2023-2024 summer science season. Will a “no-COVID” status for these isolated facilities be sought before the onset of the 2024 winter period? If so, how will this be achieved? Subcommittee members also share concern that the effectiveness of deep field camps and science/support teams would be negatively impacted if identified COVID-positive individuals are made to return to McMurdo Station for isolation, as required in the current draft USAP COVID management plan. Were this to be implemented for West Antarctic deep field science (e.g. WAIS Divide and camps beyond), teams could lose individuals for weeks due to weather and mechanical delays known to challenge already limited operations in this region.- Are protocols likely to be effective in achieving those goals? Including high altitude locations such as the South Pole and some field camps?
The Subcommittee recognizes that the scientific worksites in Antarctica have variable local resources for isolation and clinical care of infected personnel and significant differences in how quickly and safely a sick or injured person can be extracted. We understand that the unnecessary removal of a single person can have a significant and lasting impact on the overall viability of a project and the well-being of remaining personnel. This understanding should guide the protocols to be implemented at each site and for each type of USAP participant.
For the South Pole, relevant factors to consider include: altitude of 10,000 ft, expected 15 day medevac duration in summer and 21-30 days in winter, the availability of singleoccupancy rooms, high-quality accommodation and medical care (unlike most structures at McMurdo station, construction of Amundsen-Scott South Pole Station was completed in 2008). Given these factors, the subcommittee endorses the following measures that were proposed by NSF: five-day masking period upon arrival; allowing COVIDpositive patients with mild symptoms to remain at Pole; isolation in singleoccupancy rooms for positive cases; working arrangements to be considered on a case-by-case basis.
The Subcommittee discussed Rapid Antigen Test (RAT) screening prior to departure from McMurdo Station, but did not reach consensus on this point. The goal of such a measure would be to filter out COVID-positive patients prior to arrival at altitude, where their condition could potentially deteriorate rapidly. Drawbacks include what has been referred to as the “double-bind” problem, where participants headed to South Pole (or deep field camps) are expected to remain COVID-free within a McMurdo Station population (7001000 people) where positivity rates are expected to be high (up to 10% or more). Instead, other members of the committee felt that it would be beneficial to allow participants to move to South Pole Station as quickly as possible, to lower the risk of exposure (smaller community, single-occupancy rooms) and operational burdens (bedspace in McMurdo). The Subcommittee suggests that NSF implement masking with N-95 or KN-95 masks for vaccinated South Pole and field camp-bound participants for the 5 days preceding their departure from McMurdo (and for any additional days caused by flight delays).
Similar challenges exist for USAP participants needing to move through McMurdo Station and on to field camps, especially deep field camps largely supported via WAIS Divide, West Antarctica. The roughly 1000-mile distance between McMurdo Station and WAIS Divide (see map, Appendix 3), and notoriously fickle weather conditions for fixed-wing flight operations in West Antarctica, increase the time and resources needed to extract any unwell or injured USAP participant from this location. For this reason, the Subcommittee recommends that deep field camp personnel who are found to be COVID positive but do not require clinical care can complete the isolation protocols without being extracted back to McMurdo Station as stated in the current draft plan. Such extractions would cause undue delay and reduction of capacity of critical science projects, particularly the logistically complex International Thwaites Glacier Collaboration as well as operations in other areas of the deep field if fixed-wing assets are repositioned to extract participants from deep field sites. Isolation of individuals is very feasible either in personal tents or in the existing heated medical tent, as demonstrated in the 2022-23 season by the single COVID-positive patient identified at WAIS Divide. COVID-positive participants at Thwaites Glacier camps/traverses (potentially located an additional 300 miles beyond WAIS Divide) could be evacuated only to WAIS DIVIDE, although this could negatively impact the ability of small deep field teams to accomplish science goals. Finally, a metric for when to potentially alter this measure is needed. This could be to monitor the number of COVID cases in a deep field camp and take additional measures if the number of patients begins to challenge the medical resources of the site. An additional suggestion would be to consider raising the level of care available at WAIS Divide, the largest/central deep field camp supporting science in West Antarctica.
The Subcommittee agrees that the elevated physical qualifications for USAP participants moving beyond McMurdo Station for one night or more, especially required current COVID vaccination/booster, are appropriate and likely effective to reduce the risk of negative COVID outcomes among USAP participants. However, the Subcommittee is concerned about the current proposal that McMurdo Station-based USAP participants need not be up to date with COVID vaccination. Although vaccinated people sometimes get infected with the virus that causes COVID, staying up to date on COVID vaccines significantly lowers the risk of getting very sick, being hospitalized, or dying from COVID. The Subcommittee recommends all USAP deployers be up to date with COVID vaccines, including boosters, according to CDC guidance. This will minimize the impact to USAP science goals, as even medical evacuation from McMurdo Station to hospital facilities in New Zealand can impact flight schedules and resources that are otherwise needed and have extremely limited capacity for unscheduled diversion.
- In the event of a sharp increase in positive cases, are response plans adequate to ensure the safety and health of deployers as well as the continued safe operation of the stations?
Section 5 of the draft Management Plan notes that if >5% of any cohort groups (Edison Chouest Offshore, Antarctic Support Contract, and grantees) test positive at a gateway location then the remaining members (who tested negative) will be required to mask for 5 days upon arrival on the vessel or the station. This response is redundant to the existing requirement that all participants mask for the first five days after arrival on station/vessel.
NSF might request cohorts proactively identify mission-critical personnel and plan for how their activities would proceed with and/or without those persons were they to become ill and/or test positive for COVID. Recent USAP cruises have been delayed due to a single mission-critical person’s need to recover from illness before a cruise could proceed. Such delays sometimes lead to cancellation of later scheduled science cruises. Perhaps standby staffing of mission critical persons at the gateway location could better ensure all planned deployments occur.
Response plans as outlined in Section 5 of the Draft COVID Management Plan are short and simplistic at present. Given the immense impact of the November 2022 “shift” as COVID began significantly affecting McMurdo Station–including science and support delays and cancellations, significant declines in morale and some loss of trust in leadership–the Subcommittee recommends drafting more extensive response plans. Not only does such an exercise provide potential plans/roadmaps to redirect the program to continue achieving goals in light of significant COVID impacts, it also provides transparency for USAP participants who will be greatly challenged by any change in the COVID management strategy.
- Are monitoring plans sufficient to serve as an early indicator of an impending increase in cases on a timeline that will allow mitigations to be enacted?
Pre-defined metrics for monitoring changes in risk over time are important for all personnel on and off-ice to ensure safety measures are responsive to the reality on the ground. The proposed metrics numbered 1 (specific evacuation circumstances), 2 (COVID medical evacuations), 3 (clinic bed occupancy), and 5 (CDC and WHO updates) outlined in the draft management plan are sound and varied and should ensure a broad range of potential scenarios could be identified, and the proposed responses are reasonable. Metric number 4 and the proposed response (KN-95 masks for 5 days on vessel/station if >5% positive cases in a gateway cohort) are not relevant as the subcommittee recommends that all personnel wear respirator or BFC for 5 days on arrival irrespective of gateway positivity, and some members of the Subcommittee question whether routine screening of all gateway personnel is appropriate in the current epidemiologic context. Additional metrics should be considered, however.
Environmental monitoring devices and procedures such as targeted wastewater surveillance is of ongoing interest at the CDC and should be considered by USAP as a tool to provide clear metrics on viral spread at McMurdo Station and possibly also the smaller South Pole and Palmer Stations. Although this is a lagging indicator, if no other widespread surveillance testing is implemented, especially for the large McMurdo Station community, having this direct information on viral spread will help support consideration of a response. We suggest contacting the CDC (National Waste Water Surveillance System) https://www.cdc.gov/nwss/index.html for more specific guidance on how systems might be implemented at all stations/vessels.
- Are there additional protocols, tools, resources, or methods that are recommended?
Because of the congregate living and working arrangements in the USAP, the risk of COVID transmission is higher in these settings compared with the general population. Therefore, we recommend implementing a layered approach in the COVID Management Plan to reduce exposures. A layered approach includes using multiple mitigation strategies to reduce the spread of disease and lower the risk of exposure. NSF can use CDC’s Guidance on Management of COVID-19 in Homeless Service Sites and in Correctional and Detention Facilities to inform COVID-19 prevention actions in USAP settings. In addition to the CDC guidance, we offer the following specific recommendations.
COVID vaccines help your body develop protection from the virus that causes COVID. Although vaccinated people sometimes get infected with the virus that causes COVID, staying up to date on COVID vaccines significantly lowers the risk of getting very sick, being hospitalized, or dying from COVID. The Subcommittee recommends all USAP deployers be up to date with COVID vaccines, including boosters, according to CDC guidance. A waiver process can be implemented to address situations when a deploying participant cannot be vaccinated (such as for medical or religious reasons).
Ventilation is one component of maintaining healthy environments and is an important COVID prevention strategy. In most cases, improving building ventilation should not require new building ventilation systems. However, ventilation system upgrades or improvements can increase the delivery of clean air and dilute potential contaminants. The Subcommittee recommends consulting experienced heating, ventilation, and air conditioning (HVAC) professionals to assess what changes to HVAC systems and equipment are appropriate for the USAP settings. CDC provides tools to improve ventilation, including improving central air filtration, using portable high-efficiency particulate air (HEPA) fan/filtration systems, and using ultraviolet germicidal irradiation (UVGI) as a supplemental treatment.
Air filtration has not yet been adequately implemented at USAP sites. The Subcommittee recommends adding air filtration in key places (for instance, in galleys, bars, lounges, and gyms where crowding is high and mask-wearing is low) is important to investigate because 1) these are crowded stations in cold environments where people spend their leisure time indoors, and 2) air filtration will help control all respiratory illnesses, not just COVID.
Isolation is used to separate people with confirmed or suspected COVID from those without COVID. The Subcommittee recommends implementing isolation requirements according to CDC Ending Isolation and Precautions for People with COVID-19: Interim Guidance. In summary, this includes:
- People who are infected but asymptomatic or people with mild COVID-19 should isolate through at least day 5 (day 0 is the day symptoms appeared or the date the specimen was collected for the positive test for people who are asymptomatic). They should wear a mask through day 10. A test-based strategy may be used to remove a mask sooner.
- People with moderate or severe COVID-19 should isolate through at least day 10. Those with severe COVID-19 may remain infectious beyond 10 days and may need to extend isolation for up to 20 days.
- People who are moderately or severely immunocompromised should isolate through at least day 20. Use of serial testing and consultation with an infectious disease specialist is recommended in these patients prior to ending isolation.
In consultation with the responsible clinical and public health personnel, individuals who are needed for essential work functions before day 6 may leave isolation for these functions as long as they wear a respirator covering when in shared indoor public spaces.
To help USAP deployers understand the isolation guidance, CDC provides a version written for a general audience which includes an isolation and exposure calculator. The Subcommittee recommends sharing these resources with deployers who isolate to help them understand the importance of isolation and when it is appropriate to end isolation.
Being able to separate people with confirmed or suspected COVID is important in stopping transmission of COVID. Because of space limitations and dormitory-style housing, isolation can be challenging to implement in USAP settings. The Subcommittee recommends evaluating novel and effective solutions to help isolate people with COVID where dedicated, private, closed rooms are unavailable. The National Institute for Occupational Safety and Health (NIOSH) provides guidance for using portable HEPA filtration systems to create expedient patient isolation rooms and ventilated headboards.
Correctly wearing a respirator can protect people from COVID and reduce the risk that a person with COVID-19 will spread it to others. Using a layered approach, including engineering (such as improved ventilation) and administrative controls (such as enhanced physical qualification process and gateway testing), reduces the need for consistent respirator or mask use. The Subcommittee recommends requiring a NIOSH-approved N95 filtering facepiece respirator as source control when an individual must exit isolation at any point through day 10 and as respiratory protection when supported by early indicators of an impending increase in cases. Additionally, the Subcommittee recommends encouraging USAP deployers to wear a respirator or barrier face covering in public indoor spaces when traveling or stationed at the gateway cities, when first arriving in Antarctica, and before transferring within Antarctica.
As much as possible, we recommend using respirators and masks that meet a standard to offer a known level of protection. Examples include NIOSH Approved® N95® filtering facepiece respirators, KN-95 filtering facepiece respirators, and Workplace Performance and Workplace Performance Plus Barrier Face Coverings. It is important to offer a variety of models to choose from, allowing deployers to identify a model that fits best to their face.
Communicate supportive workplace policies clearly, frequently, tailored to all stakeholders (internal and external to USAP) and via multiple methods. The Subcommittee recommends supplementing workers’ normal and required job training with additional training and information about COVID-19, recognizing signs and symptoms of infection, and ways to prevent exposure to the virus. In addition, training should include information on how to implement the COVID-19 Management Plan. OSHA provides additional information about training in Protecting Workers: Guidance on Mitigating and Preventing the Spread of COVID-19 in the Workplace.
Given the significant impact of the “shift” in the 2022-2023 field season (the two week travel shutdown for new participants coming into USAP facilities) and its apparent connection to public revelations of a COVID outbreak at McMurdo Station, NSF should consider communicating publicly about their plan and intentions for balancing COVID risk with operational capacity needed to accomplish priority science in Antarctica. Clear and consistent communication on the status of COVID in USAP facilities (as much as is known) should also be shared with all levels of leadership within NSF to mitigate reactive decision making that can have widespread and lasting impact on science and support needs for the USAP as well as damaging effectiveness of leadership within USAP.
The Subcommittee recommends ensuring that small numbers of COVID-positive (but vaccinated) patients not requiring clinic-level care be allowed to isolate in deep field camps (e.g. WAIS Divide) rather than being extracted back to McMurdo as stated in the current draft plan (see related response to Question 3). The roughly 1000 mile distance between McMurdo Station and WAIS Divide (see map in Appendix 3), and notoriously fickle weather conditions for fixed-wing flight operations in West Antarctica, increase the time and resources needed to extract any unwell or injured USAP participant from this location. This added effort required to both get USAP participants to WAIS Divide (and beyond) to accomplish science goals must be weighed against the similar effort to extract them. While extracting any COVID-positive participant is the most conservative approach as far as medical risk, this approach is not conservative with respect to its likely impact on field science and support teams’ ability to complete their science goals for the season. These small teams, under the current COVID protocols (removing COVID-positive deep field participants for isolation at McMurdo Station), would potentially lose team members for the 5 days of isolation required at McMurdo Station and then however many additional days it takes to get that participant back to WAIS Divide due to mechanical, weather, and flight scheduling/priority delays. It could take the entire 5 day isolation period just for an aircraft to reach WAIS Divide from McMurdo Station.
Appendix 1. Membership, Subcommittee on USAP COVID Protocols
- Dr. Peter Neff, Glaciologist, University of Minnesota (Subcommittee Chair)
- Dr. Phil Bart, Geologist, Louisiana State University*
- Cdr. Sam Blase, U.S. Coast Guard Liaison to NSF
- Dr. Marion Dierickx, Astrophysicist, Harvard
- Capt. Chad Dowell, Deputy Associate Director for Emergency Preparedness and Response, CDC/NIOSH
- Dr. Tenagne Haile-Mariam, Associate Professor of Emergency Medicine, GWU
- Dr. Donald Kosiak, Chief Medical Officer, Leidos
- Dr. Lori Newman, Division of Microbiology & Infectious Diseases, NIH/NIAID
- Col. Brendan Noone, Chief, Aerospace Medicine Division, Pacific Air Forces
- Dr. Sara Sawyer, Virologist, University of Colorado-Boulder
- Dr. Jade Spurgeon, Director of Health and Medical Systems, NASA
*Member of OPP Advisory Committee
Appendix 2. Subcommittee Charge
National Science Foundation
Advisory Committee for Polar Programs
Subcommittee on the USAP COVID Protocols
Subcommittee Charge
- Subcommittee’s Official Designation: The National Science Foundation (NSF) Advisory Committee for Polar Programs, Subcommittee on the U.S. Antarctic Program (USAP) COVID Protocols (the Subcommittee).
- Authority: The Subcommittee is established in accordance with Section 13 of the charter for the NSF Advisory Committee for Polar Programs.
- Objective and Scope of Activities: The Subcommittee provides advice and recommendations concerning the USAP development and implementation of health protocols in response to COVID in USAP-operated sites in Antarctica.
- Description of Duties: The Subcommittee shall review the drafted COVID posture and provide additional recommendations to reduce the risk COVID presents to the logistical operations and science support of the USAP, operated by the Office of Polar Programs, Directorate for Geosciences (GEO). In accordance with Section 13 of the charter for the NSF Advisory Committee for Polar Programs (the Committee), the Subcommittee shall report their recommendations and advice to the full Committee for deliberation and discussion.
- Membership: The Subcommittee shall have no more than 12 members appointed by the Director of the Office of Polar Programs. At least one member of the Subcommittee shall also be a member of the NSF Advisory Committee for Polar Programs (AC-OPP). Subcommittee members shall be selected to provide balanced representation of the USAP community, medical and research community, and other National Antarctic Programs. To the extent practicable, effort shall be made to achieve a diverse membership that includes individuals from different fields, as well as underrepresented groups.
- Subcommittee Chair: The Director of the Office of Polar Programs shall appoint the Subcommittee Chair.
- Designated NSF Official: The Office of Polar Programs will appoint a designated NSF official for the Subcommittee. The Designated Federal Official calls the Subcommittee meetings, prepares meeting agendas, and attends Subcommittee meetings.
- Meetings: The Subcommittee shall meet at least once.
- Working Groups: The Subcommittee may not form Working Groups for any purpose.
- Duration: It is expected that the Subcommittee shall continue until a final recommendation report is provided to the AC-OPP, or until the AC-OPP is disbanded, whichever occurs first.
- Approval: The Director of the Office of Polar Programs shall be required to approve the Subcommittee Charge, including any subsequent changes, upon the recommendation of the Subcommittee.
- Minutes: The Subcommittee shall maintain minutes of all meetings and provide those minutes to the NSF Advisory Committee for Polar Programs.
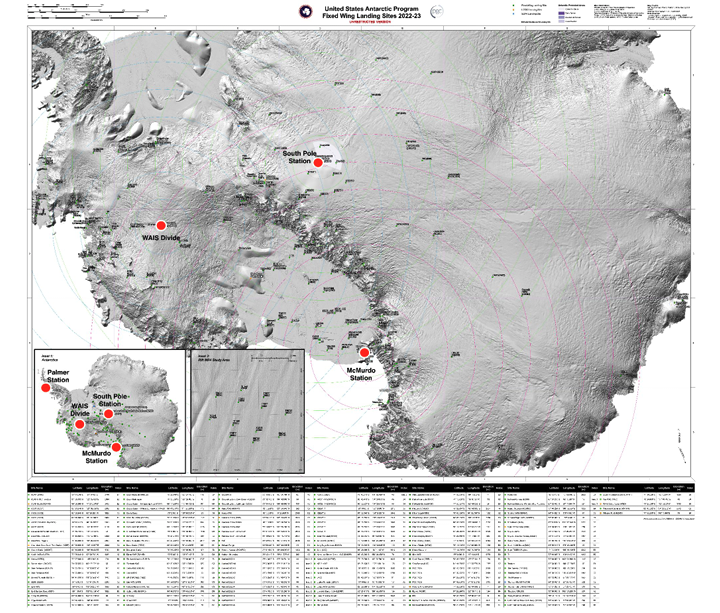
Appendix 3. USAP Fixed Wing Landing Sites 2022-23 (Major USAP facilities mentioned in text annotated for reference)
{kind=link}
Annotated to show location of year-round USAP stations and the large deep field camp WAIS Divide (red dots) and the range of locations possibly visited by USAP participants. The original map was produced by the Polar Geospatial Center.